SpineUniverse Case Study Library
History
The patient is a 14-year-old healthy, high-level gymnast who presented with one-year history of insidious low back pain. The pain was associated with physical activities and worsened with impact activities. She described recent (past few months) onset of pain and tingling down her left leg to the dorsum of the left foot.
Examination
- 5′-3″, 140-pound female
- Limited range of motion in the lumbar spine
- Pain with >40 degrees of forward flexion and >10 degrees of extension
- 5/5 strength throughout lower & upper extremities
- Sensation intact to pin prick from C4-T1 and L2-S1
- Patellar and achilles deep tendon reflexes: 2+
- No upper motor neuron signs
Prior Treatment
She had undergone multiple trials of physical therapy and chiropractic modalities, experiencing no improvement in symptoms.
Pretreatment Imaging
Anteroposterior (AP) and lateral standing lumbar radiographs reveal a Grade III spondylolisthesis of L5 on S1 (Figures 1A and 1B, below).
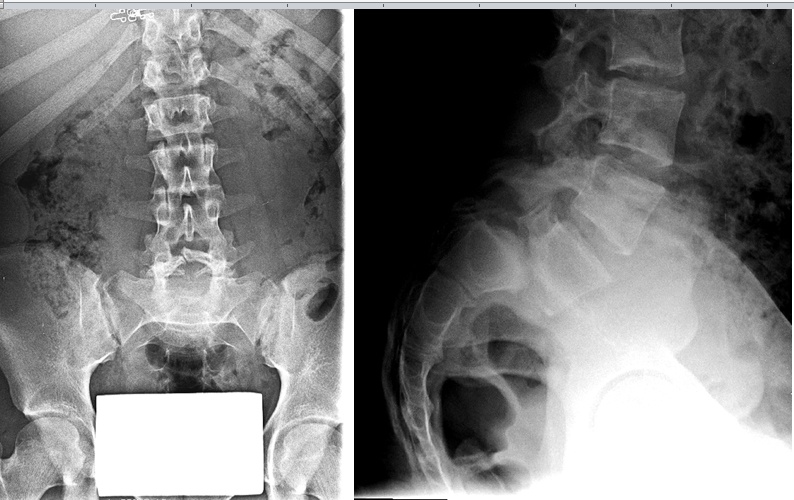
Figures 1A and 1B (above)
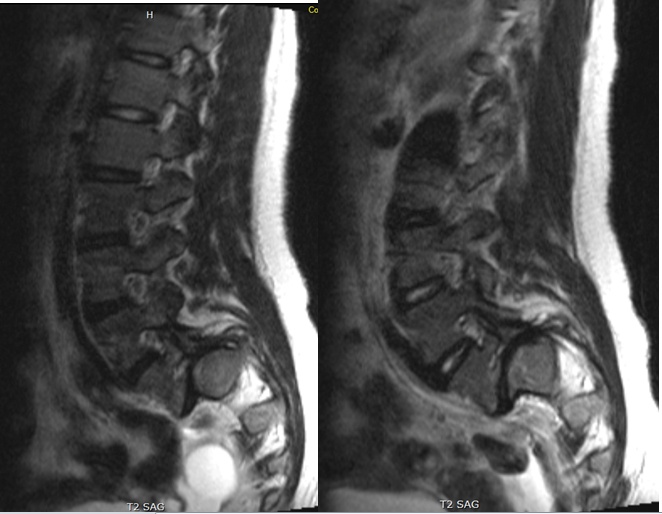
Figures 2A and 2B (below) show axial and sagittal T2-weighted MRI sequences reveal:
- Exaggerated lumbar lordosis
- Grade III spondylolisthesis, L5-S1
- Bilateral spondylolysis, L5
- Mild posterior wedging of L5 and mild deformity of the superior S1 endplate
- Severe stenosis at L5-S1 of the spinal canal and neural foramina

Figures 2A and 2B (above)
Left and right paraspinal T2-weighted MRI sequences (Figures 3A and 3B, below) reveal severe stenosis at L5-S1, neural foramina.
Figures 3A and 3B (above)
Diagnosis
High-grade (Myerding Grade III) isthmic spondylolisthesis
Selected Treatment
In-situ circumferential L4-S1 fusion.
- L4-L5 posterior spinal decompression, laminectomy
- L5-S1 bilateral lateral recess and foraminal decompression
- Sacral dome osteotomy
- Transforaminal lumbar interbody fusion (TLIF) L5-S1
- Posterior segmental pedicle screw instrumentation with rod placement L4-S1
- Posterior spinal fusion autograft and allograft L4-S1
Intra-operative findings:
- Right L5 nerve root appeared significantly stretched
- Left L5 nerve root compressed by hypertrophic ligament and capsule -> impingement of the exiting nerve root
Post-Treatment Imaging
Postoperative standing AP (Figure 4A), lateral radiographs of the lumbar spine (Figure 4B) and lumbo-sacral junction (Figure 4C). Successful fusion observed with cage in adequate position at the L5-S1 junction with instrumentation intact from L4 to sacrum.
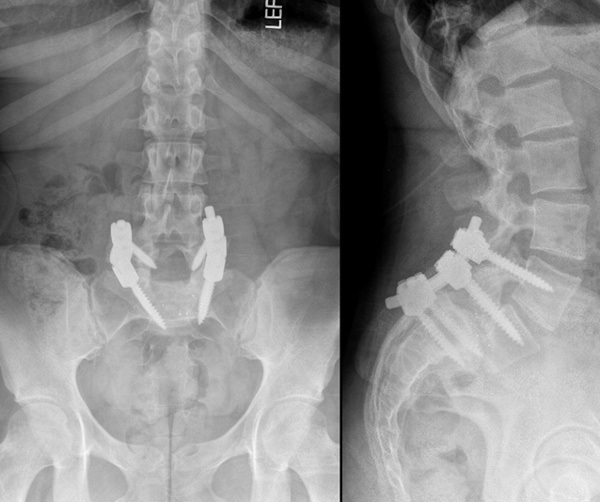
Figures 4A and 4B (above)
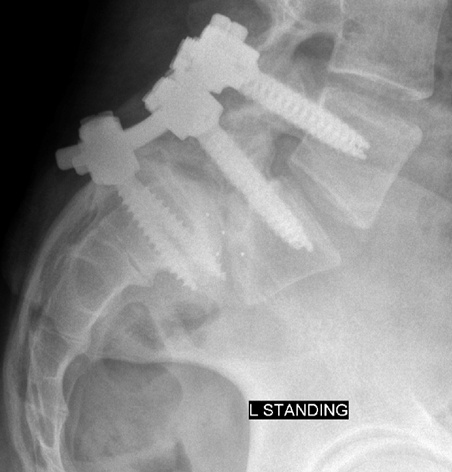
Figure 4C (above)
Outcome
At 2-years following surgery, the patient has returned to gymnastics and cheerleading with no back or leg pain. She is even able to run one-mile in nine minutes without any problems.
Case Discussion
Of note as well, is partial but not complete reduction. This was probably obviated intraoperatively by finding the nerve roots already stretched. This is often the case despite complete bilateral facetectomy and disc space mobilization, and it is preferable to bilateral L5 deficits. This would be a challenging case from an anterior approach, and the authors impart many thoughtful and appropriate messages with this case. The enemy of good is better.